
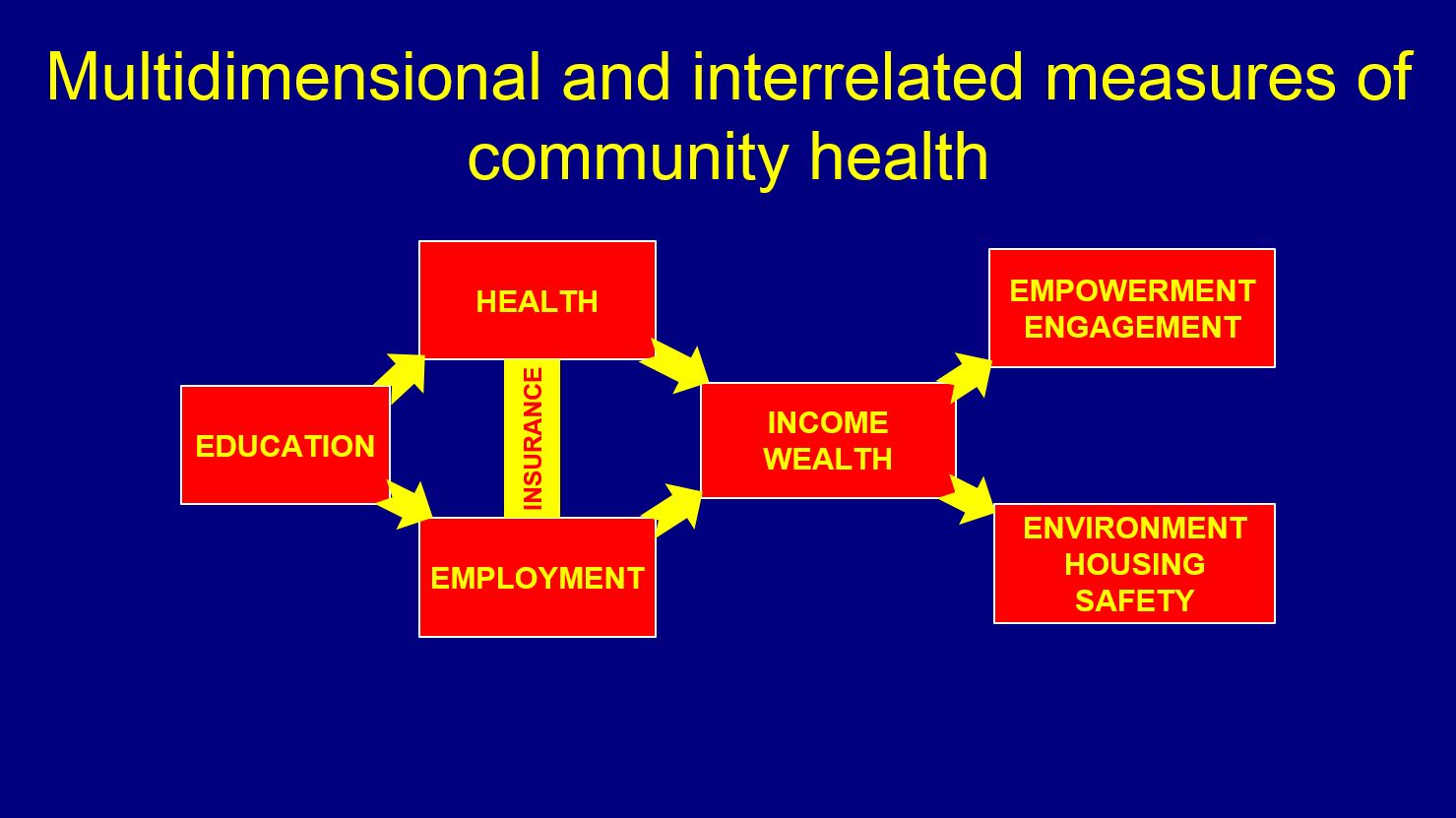
 Figure 1: Multidimensional and interrelated measures of community health. Image by Frank FranklinFrank A. Franklin, M.D., M.P.H., Ph.D. - Professor and Chair, Department of Maternal and Child Health, School of Public Health
Figure 1: Multidimensional and interrelated measures of community health. Image by Frank FranklinFrank A. Franklin, M.D., M.P.H., Ph.D. - Professor and Chair, Department of Maternal and Child Health, School of Public Healthfrankln@uab.edu
Dear Students,
The United States, among similar high-income countries, ranks low on many health measures (e.g., infant and maternal mortality). Also, within the U.S., there are twofold differences in these health measures between whites and African-Americans. Socioeconomic factors, such as education, employment, wealth and family/social support, and personal health behaviors like diet and exercise, unsafe sex and the use of alcohol and tobacco account for 70 percent of these deficits and inequities while health care (e.g. access to care and quality of care) is responsible for only 20 percent. Hence, a larger view of community health includes multidimensional and interrelated measures such as income, employment, education and training, health care, housing, income segregation, neighborhood crime, and civic empowerment and social engagement (see Figure 1). By these measures, I diagnose the city of Birmingham as being in very poor community health.
We have powerful therapeutic agents for improving the health of the city of Birmingham. However, they are not used at high enough doses and for sufficient duration. These agents are eds and meds that are anchored in our community by their mission, invested capital, sizeable footprint and fixed assets. Birmingham’s eds and meds include UAB, the UAB Health System, Children’s of Alabama and St. Vincent’s Hospital with their vast economic, human and social capital. They have replaced manufacturing to become the largest employer in our community and are the region’s largest purchaser of goods and services.
Birmingham’s downtown is experiencing a commercial and entertainment renaissance extending from Uptown to Southside and east to Avondale and Woodlawn. The time is opportune for the development of new community health initiatives throughout the city of Birmingham. Currently, Birmingham’s eds and meds provide essential health care, social services, employment and university education. Yet many potential roles for eds and meds for community health are weak and can be initiated, enhanced and expanded. Anchor institutions have the economic potential to leverage their assets and revenues to promote local economic development through such strategies as directing a greater percentage of their purchasing power toward local vendors, hiring a greater percentage of their workforce locally, providing capital for community nonprofits, entrepreneurs and employee-owned firms and developing holistic community schools.
These larger roles of eds and meds in community health and wealth building are ongoing in many communities. Local procurement and hiring, enterprise accelerators and employee owned enterprises have had powerful economic development impacts in Cleveland and Philadelphia. In Cleveland, the Cleveland Foundation initiated an anchor institution collaborative strategy involving universities, hospitals and cultural institutions. Similarly, the University of Pennsylvania has made major investments in West Philadelphia. In Cleveland, local procurement fuels an efficient model of large-scale worker-owned and community-benefiting businesses. A network of three non-profits employs low-income residents from inner-city Cleveland. These cooperatives are networked together with a central non-profit corporation holding company that helps them with finances and management assistance.
This link between anchor institutions and community wealth building is catalyzed by community development financial institutions (CDFIs). Along with the economic development from university purchasing and hiring, anchor institutions provide capital or low-interest loan financing through CDFIs. They provide credit, financial services and low-interest loans for low-income people and communities underserved by mainstream commercial banks and lenders. These economic development services support the start and growth of small businesses and affordable housing. In turn, small business ownership fuels the growth of the local economy.
Developing year-round, holistic, community schools open for the whole community has been a major initiative of eds and meds in Cincinnati. In a holistic model, integrated services (e.g. physical and mental health, expanded learning times, parent education, family counseling and social services) support students, families, schools and communities to target students’ academic and non-academic outcomes. Cincinnati Public Schools created Community Learning Centers (CLCs) to strengthen links between schools and communities, support student achievement and revitalize neighborhoods while functioning as hubs where partnerships implement the holistic model. All partnerships must be financially self-sustaining without dependence upon the school budget. Partners include the city school system and health department, United Way, Community Foundation, YMCA, Children’s Hospital Medical Center and the University of Cincinnati. In less than a decade, CLCs cost effectively increased high school graduation rates from 51 percent to 83 percent and narrowed the achievement gap between African-American and white students from 14.5 percent to 4.3 percent.
Keystones of the eds and meds community health and wealth development model are local procurement, local hiring, providing funding for CDFIs and developing CLCs. Anchor institutions engage in community development because it is good business to expand the social and economic progress of the surrounding community. It is also in their enlightened self-interest. Finally, there are “carrots” such as grants and “sticks” such as IRS requirements under the Affordable Care Act (ACA). As part of ACA, nonprofit hospitals for their federal tax exempt status must perform a community health needs assessment and implement and evaluate a strategy to address community health needs. As ACA expands health insurance coverage, the need for direct financial assistance for patient care as their community contribution may decline. Thus, expanded health insurance coverage permits a potential shift of meds community benefit from direct patient care to community health and wealth building activities. Natural collaborators in our community along with eds and meds are the other types of nonprofit anchor institutions like the Community Foundation, other locally-focused philanthropies, faith-based institutions, cultural institutions such as museums, United Way and community colleges. This collaboration can be facilitated by leadership at our eds and meds. The use of these therapeutic agents by this collaboration can efficiently and effectively heal our poor community health and wealth.
The United States, among similar high-income countries, ranks low on many health measures (e.g., infant and maternal mortality). Also, within the U.S., there are twofold differences in these health measures between whites and African-Americans. Socioeconomic factors, such as education, employment, wealth and family/social support, and personal health behaviors like diet and exercise, unsafe sex and the use of alcohol and tobacco account for 70 percent of these deficits and inequities while health care (e.g. access to care and quality of care) is responsible for only 20 percent. Hence, a larger view of community health includes multidimensional and interrelated measures such as income, employment, education and training, health care, housing, income segregation, neighborhood crime, and civic empowerment and social engagement (see Figure 1). By these measures, I diagnose the city of Birmingham as being in very poor community health.
We have powerful therapeutic agents for improving the health of the city of Birmingham. However, they are not used at high enough doses and for sufficient duration. These agents are eds and meds that are anchored in our community by their mission, invested capital, sizeable footprint and fixed assets. Birmingham’s eds and meds include UAB, the UAB Health System, Children’s of Alabama and St. Vincent’s Hospital with their vast economic, human and social capital. They have replaced manufacturing to become the largest employer in our community and are the region’s largest purchaser of goods and services.
Birmingham’s downtown is experiencing a commercial and entertainment renaissance extending from Uptown to Southside and east to Avondale and Woodlawn. The time is opportune for the development of new community health initiatives throughout the city of Birmingham. Currently, Birmingham’s eds and meds provide essential health care, social services, employment and university education. Yet many potential roles for eds and meds for community health are weak and can be initiated, enhanced and expanded. Anchor institutions have the economic potential to leverage their assets and revenues to promote local economic development through such strategies as directing a greater percentage of their purchasing power toward local vendors, hiring a greater percentage of their workforce locally, providing capital for community nonprofits, entrepreneurs and employee-owned firms and developing holistic community schools.
These larger roles of eds and meds in community health and wealth building are ongoing in many communities. Local procurement and hiring, enterprise accelerators and employee owned enterprises have had powerful economic development impacts in Cleveland and Philadelphia. In Cleveland, the Cleveland Foundation initiated an anchor institution collaborative strategy involving universities, hospitals and cultural institutions. Similarly, the University of Pennsylvania has made major investments in West Philadelphia. In Cleveland, local procurement fuels an efficient model of large-scale worker-owned and community-benefiting businesses. A network of three non-profits employs low-income residents from inner-city Cleveland. These cooperatives are networked together with a central non-profit corporation holding company that helps them with finances and management assistance.
This link between anchor institutions and community wealth building is catalyzed by community development financial institutions (CDFIs). Along with the economic development from university purchasing and hiring, anchor institutions provide capital or low-interest loan financing through CDFIs. They provide credit, financial services and low-interest loans for low-income people and communities underserved by mainstream commercial banks and lenders. These economic development services support the start and growth of small businesses and affordable housing. In turn, small business ownership fuels the growth of the local economy.
Developing year-round, holistic, community schools open for the whole community has been a major initiative of eds and meds in Cincinnati. In a holistic model, integrated services (e.g. physical and mental health, expanded learning times, parent education, family counseling and social services) support students, families, schools and communities to target students’ academic and non-academic outcomes. Cincinnati Public Schools created Community Learning Centers (CLCs) to strengthen links between schools and communities, support student achievement and revitalize neighborhoods while functioning as hubs where partnerships implement the holistic model. All partnerships must be financially self-sustaining without dependence upon the school budget. Partners include the city school system and health department, United Way, Community Foundation, YMCA, Children’s Hospital Medical Center and the University of Cincinnati. In less than a decade, CLCs cost effectively increased high school graduation rates from 51 percent to 83 percent and narrowed the achievement gap between African-American and white students from 14.5 percent to 4.3 percent.
Keystones of the eds and meds community health and wealth development model are local procurement, local hiring, providing funding for CDFIs and developing CLCs. Anchor institutions engage in community development because it is good business to expand the social and economic progress of the surrounding community. It is also in their enlightened self-interest. Finally, there are “carrots” such as grants and “sticks” such as IRS requirements under the Affordable Care Act (ACA). As part of ACA, nonprofit hospitals for their federal tax exempt status must perform a community health needs assessment and implement and evaluate a strategy to address community health needs. As ACA expands health insurance coverage, the need for direct financial assistance for patient care as their community contribution may decline. Thus, expanded health insurance coverage permits a potential shift of meds community benefit from direct patient care to community health and wealth building activities. Natural collaborators in our community along with eds and meds are the other types of nonprofit anchor institutions like the Community Foundation, other locally-focused philanthropies, faith-based institutions, cultural institutions such as museums, United Way and community colleges. This collaboration can be facilitated by leadership at our eds and meds. The use of these therapeutic agents by this collaboration can efficiently and effectively heal our poor community health and wealth.

