Case History
Placenta at 21 weeks. Most likely diagnosis?
- Choriocarcinoma
- Complete Hydatidiform Mole
- Partial Hydatidiform Mole
- Placental Mesenchymal Dysplasia
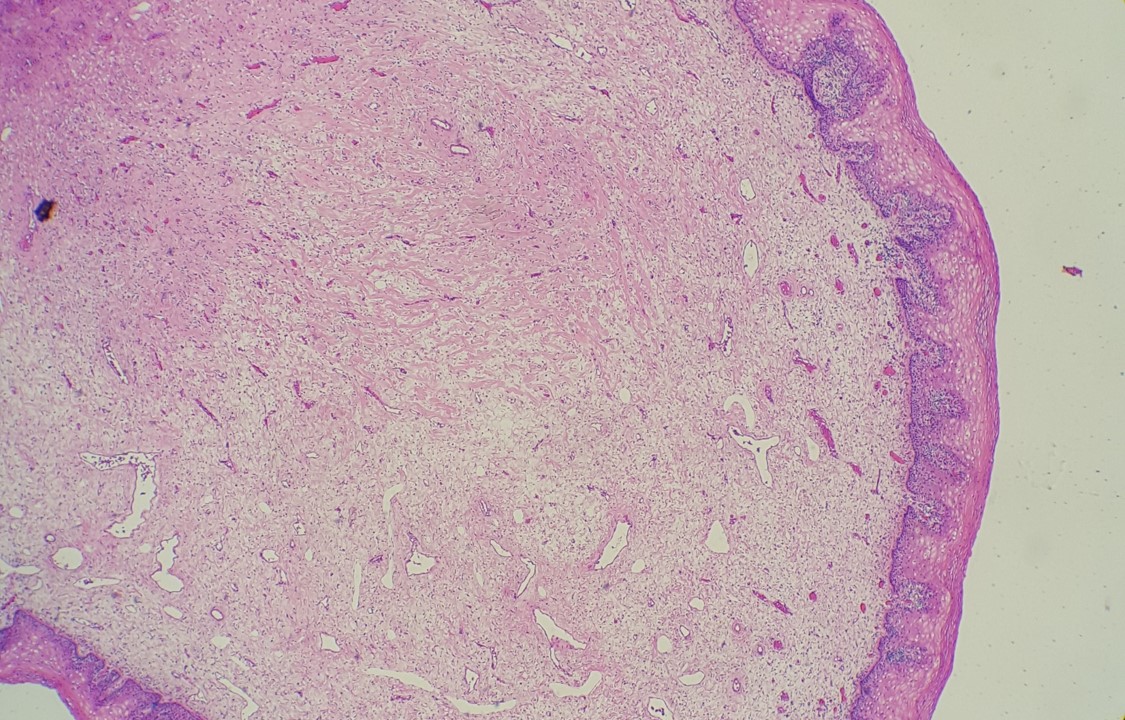



Answer: B. Complete Hydatidiform Mole
Discussion: This placenta was one of 2 separate discs of a diamniotic, dichorionic twin pregnancy. The patient requested expectant management, but eventually underwent cesarean section in the setting of preterm labor. Other gestational complications included pre-eclampsia and hyperthyroidism in this case. The non-affected placenta and fetus were structurally normal, but previable.
The pathologic features in this case are diagnostic of complete hydatidiform mole. Complete moles are characterized by markedly hydropic villi which may grossly resemble a “bunch of grapes.” Histologically, this is evidenced by diffusely enlarged villi with central cistern formation and circumferential trophoblastic hyperplasia, which may be exuberant. Loss of p57KIP2 expression in villous stroma and cytotrophoblast is diagnostic. No fetal tissues are present in association with a complete mole.
In contrast, partial hydatidiform mole is characterized by villi of varying size and shape with scalloping of the villous borders and variably hydropic changes. Trophoblast hyperplasia tends to be less prominent than in complete moles. Because of the irregular scalloped borders, invaginations may be transected tangentially, giving rise to trophoblastic “pseudoinclusions”. Nuclei of villous stromal cells and cytotrophoblast classically retain p57 staining. Fetal tissue may be present in these specimens.
Complete moles are nearly always diploid, and karyotype may be either 46,XX or 46,XY. This typically arises from endoreduplication (duplication without mitosis) of a single sperm after fertilization of an empty ovum, or less commonly, dispermic fertilization of an empty ovum. In either case, because the ovum is anucleate, there is no maternal genetic material. Because P57KIP2 (a cyclin dependent kinase inhibitor) is expressed from the maternally inherited allele and silenced on the paternal allele, this accounts for the loss of p57KIP2 in complete moles.
Partial moles are typically triploid and either 69,XXX or 69,XXY. This usually arises from dispermic fertilization of a normal ovum. Because both maternal and paternal material are present, p57KIP2 expression in villous stroma and cytotrophoblast is retained.
Complete mole is less common than partial, occurring at a rate of about 1/1000 pregnancies, but the rate of persistent gestational trophoblastic disease (GTD) is higher (15-20% of cases). Partial mole occurs about 3/1000 pregnancies with a rate of persistent GTD only 0.2-4% of cases. Thus the identification of complete mole, and clinicopathologic distinction between complete and partial mole, is important. Multiple gestation involving a complete mole and coexisting normal fetus is rare, approximating 1/20,000-100,000 pregnancies. Complications are increased in this situation and include pre-eclampsia and hyperthyroidism, as were seen in this case. Other complications include spontaneous abortion or IUFD of the normal fetus.
References:
- Ronnett BM. Hydatidiform Moles: Ancillary Techniques to Refine Diagnosis. Arch Pathol Lab Med. 2018 Dec;142(12):1485-1502.
- McConnell TG, Murphy KM, Hafez M, et al. Diagnosis and subclassification of hydatidiform moles using p57 immunohistochemistry and molecular genotyping: validation and prospective analysis in routine and consultation practice settings with development of an algorithmic approach. Am J Surg Pathol. 2009 Jun;33(6):805-17.
- Lin LH, Maestá I, Braga A, et al. Multiple pregnancies with complete mole and coexisting normal fetus in North and South America: A retrospective multicenter cohort and literature review. Gynecol Oncol. 2017 Apr;145(1):88-95.
Case contributed by: Virginia Duncan, M.D., Assistant Professor, Anatomic Pathology