Case History
A 39-year-old female with abnormal vaginal bleeding, history of abnormal Pap smears, and LEEP for HSIL. The patient had a full term delivery two years ago. Hysterectomy was performed. Section of the lower uterine segment is illustrated.
- Intermediate trophoblastic tumor (epithelioid trophoblastic tumor)
- Squamous cell carcinoma
- Placental site nodule
- Exaggerated placental site
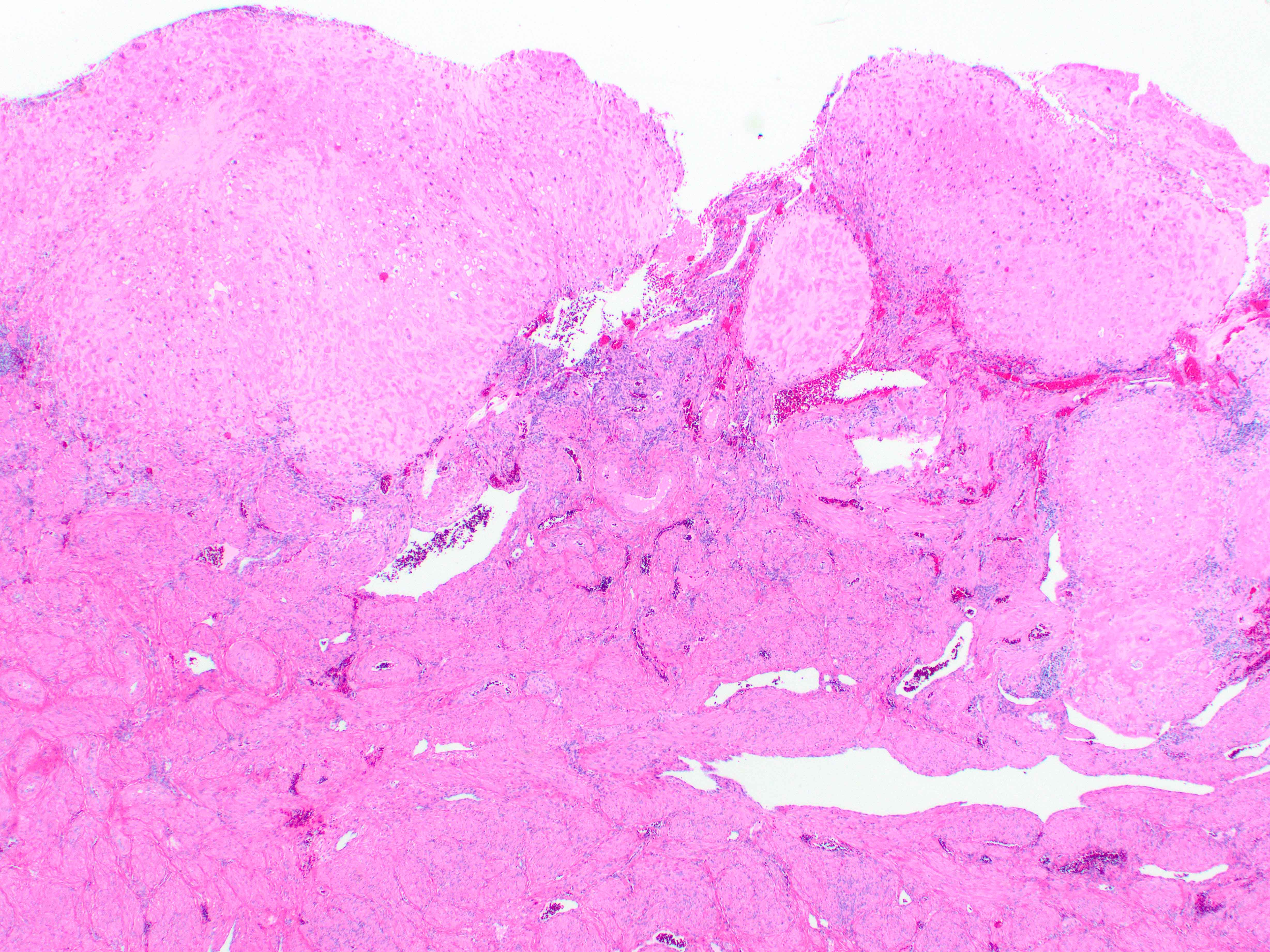
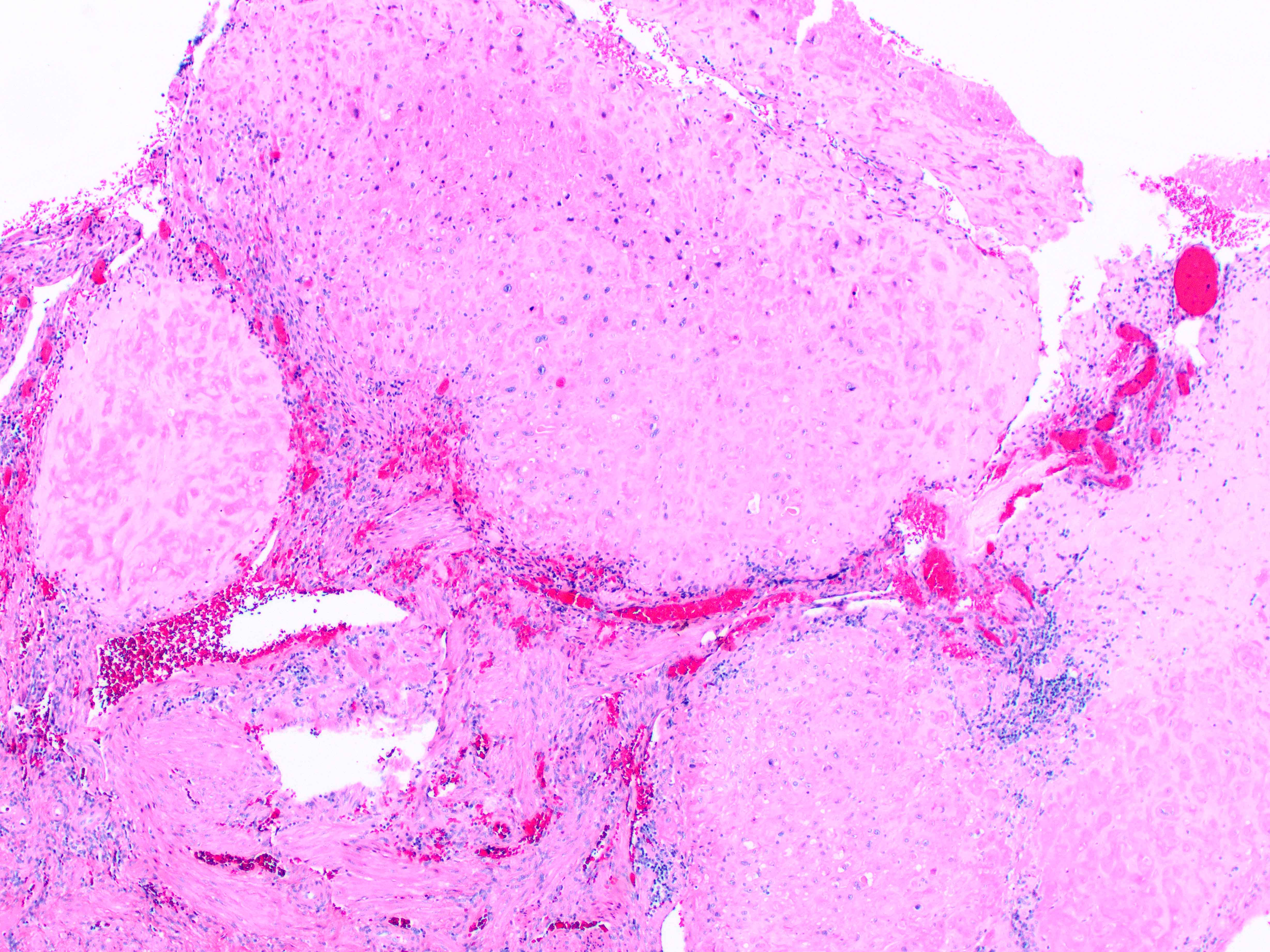
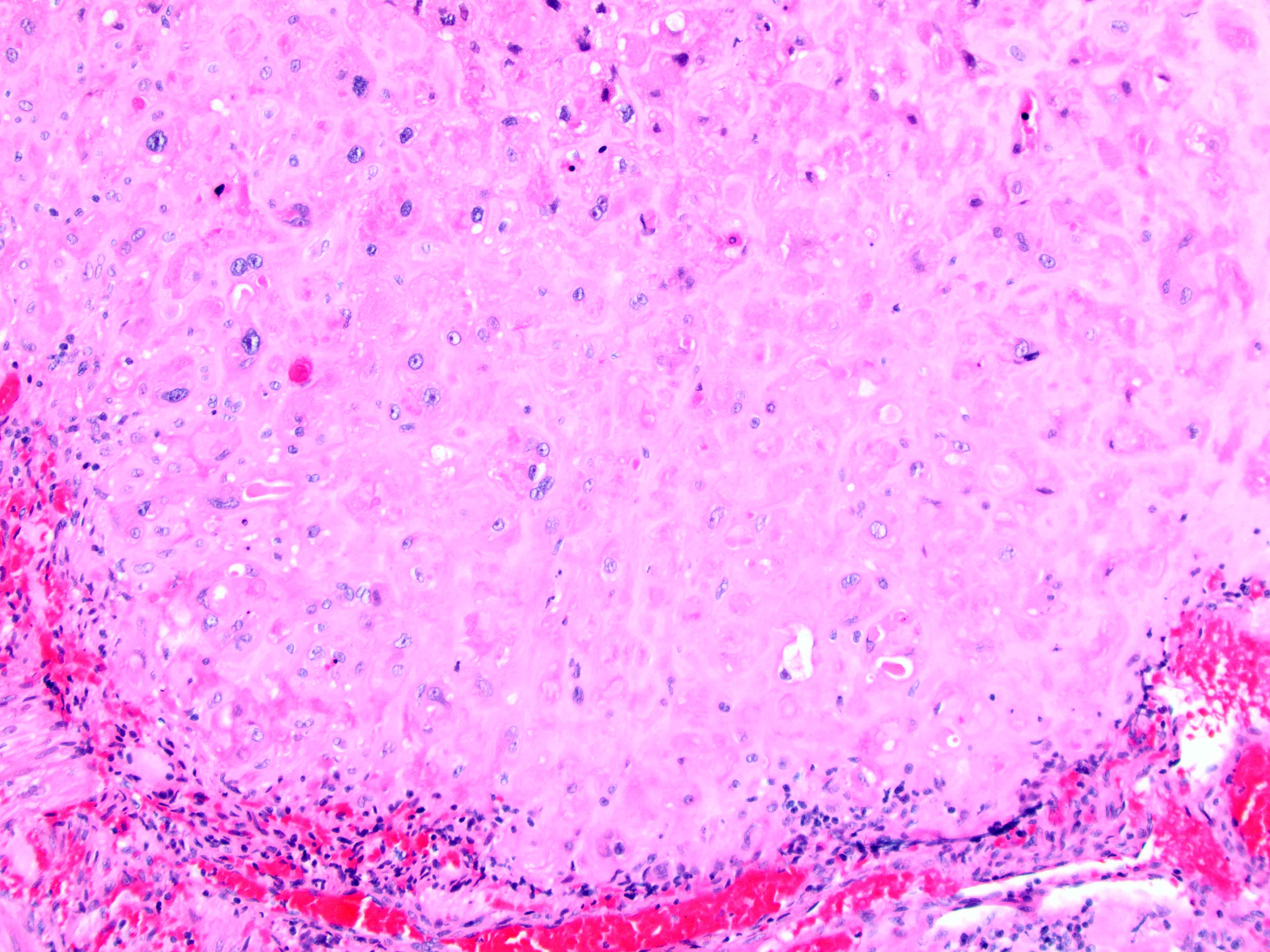
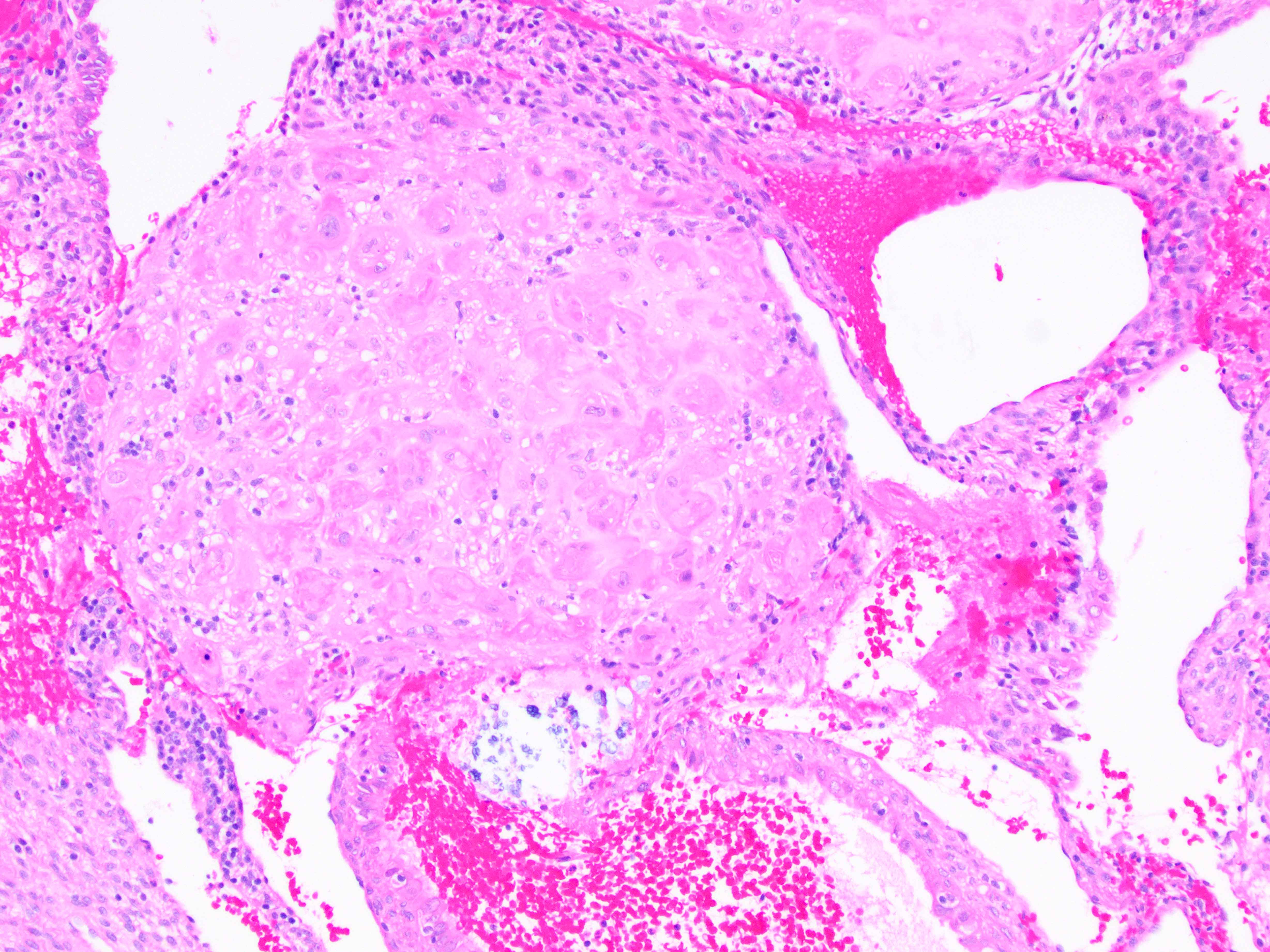
Correct answer: “C,” Placental site nodule.
These lesions were originally described as placental site nodules or plaques. It is composed of nodular aggregates of mononuclear intermediate trophoblastic cells embedded in a hyalinized stroma. Mitotic activity is generally absent. It is a benign lesion that is thought to represent a portion of uninvoluted placental site from remote gestation in the uterus. It is considered a benign counterpart of epithelioid trophoblastic tumor, but lacks the diagnostic criteria required for the latter; i.e. large areas of geographic necrosis, calcifications, and occasional mitotic figures. The differential diagnosis with high-risk HPV-related lesion (squamous cell carcinoma) is relevant, particularly, in light of the history. A small panel of immunohistochemical stains (p16 and CK18) has been suggested to resolve morphologically equivocal cases, especially in biopsy or curettage specimens. The diagnosis of exaggerated placental site (EPS) is typically made in a setting of recent gestation. In addition to the mononuclear cell component, EPS is characterized by an increased number of multinucleated implantation site intermediate trophoblastic cells often infiltrating between muscle bundles.
References:
Kurman RJ, Ellenson LH, Ronnett BM, eds. Blaustein’s Pathology of the Female Genital Tract 6th ed. New York NY: Springer; 2011:1121-1126.
Case contributed by: Anna Yemelyanova, M.D., Professor, Anatomic Pathology