Case History
The patient is a 23-month-old female with status post liver transplant one month ago due to biliary atresia and shows newly elevated liver function test. The liver biopsy is performed and the histological findings [Figure 1 (medium power at upper right corner) and Figure 2 (high power at lower right corner)] are below.
What is your diagnosis?
- Acute cellular rejection
- Histoplasmosis
- CMV infection
- Adenovirus infection
- HSV infection
- Centrizonal necrosis due to ischemia
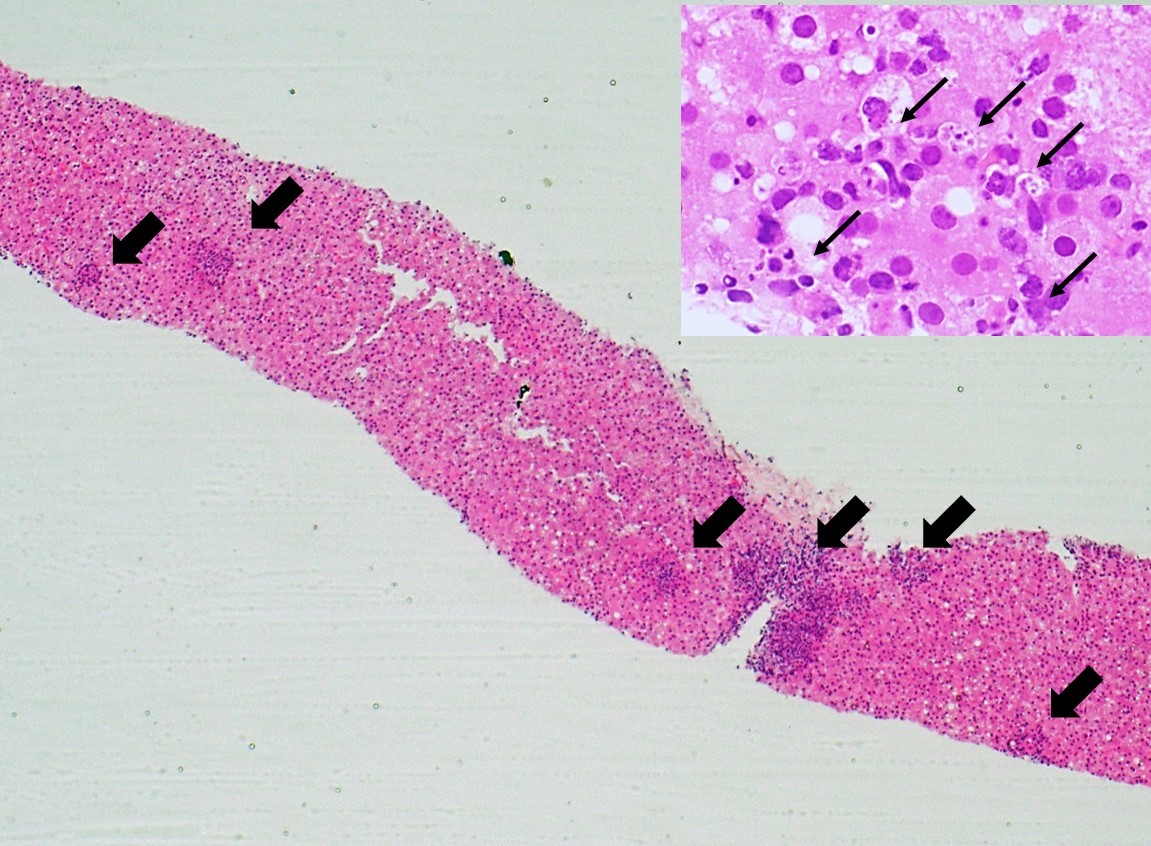
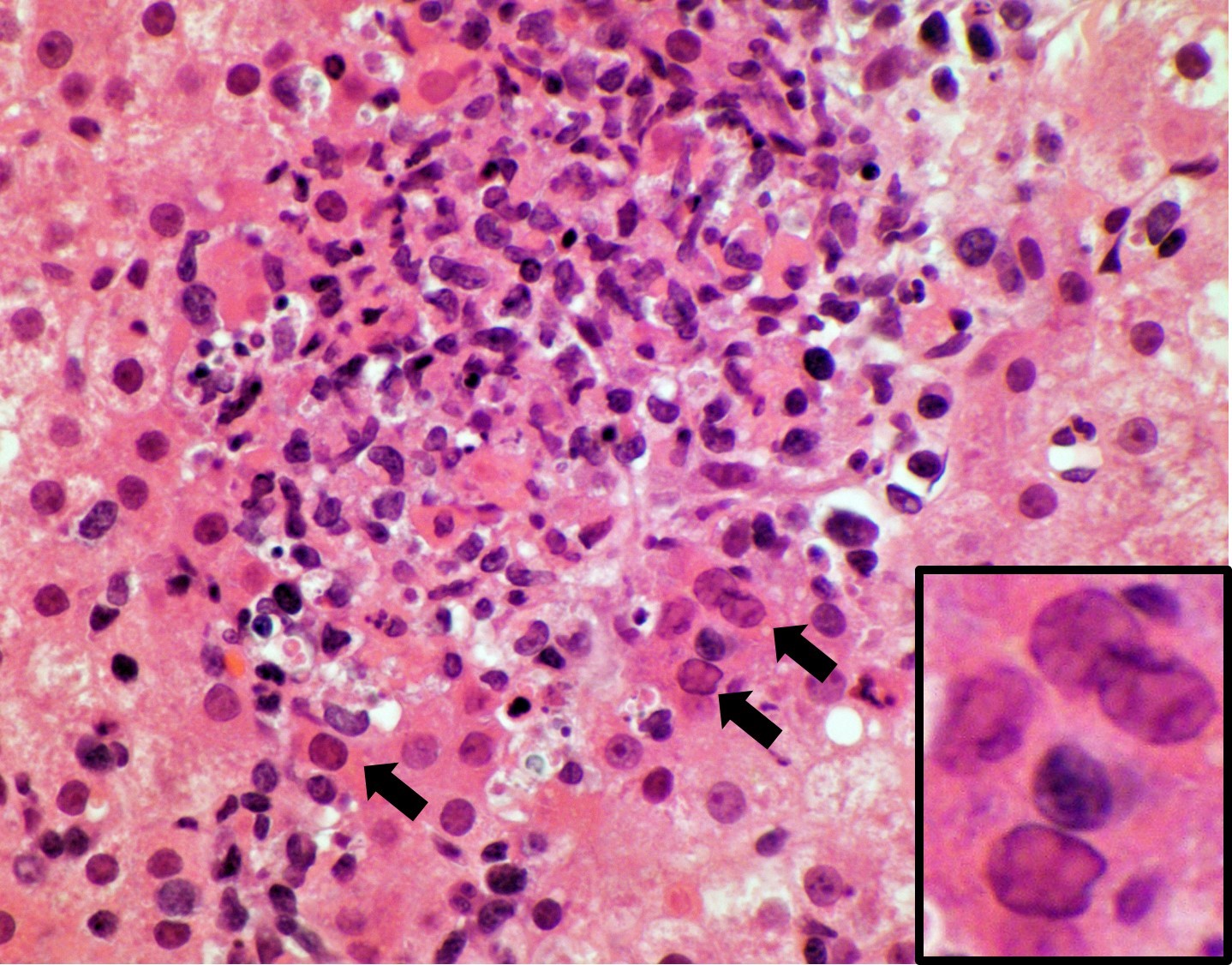
Figure 1. Low power shows multiple inflammatory foci within the lobule. The inset (medium power at upper right corner) shows spotty necrosis/apoptosis with nuclear debris and inflammatory cells consisting of histiocytes, lymphocytes, and rare eosinophils.
Figure 2. Nuclear inclusions within the hepatocytes are present at the edge of an inflammatory/necrotic focus. The inset (high power) at lower right corner reveals glassy or smudgy nuclear inclusions with central eosinophilic appearance.
Answer: D. Adenovirus infection

Figure 3. An immunohistochemical stain for adenovirus is positive (predominantly nuclear withsome cytoplasmic positivity).
Occasionally, a virus more often associated with infection of other organs (e.g., HSV or adenovirus) can give rise to a severe hepatitis. Characteristic features of adenovirus infection in the liver hepatocyte necrosis, ranged from spotty to massive, and smudged to glassy intranuclear inclusions within hepatocytes. The necrosis is usually non-zonal as well as the periportal region. Associated inflammation is lymphohistiocytic; no neutrophilic inflammation is identified. These inclusions were most commonly present at the edges of areas of necrosis, but occasionally were also scattered throughout the lobule. Although these inclusions were predominantly basophilic, several cases demonstrated inclusions with glassy eosinophilic areas as well. Notably, the biliary epithelium can be infected.
In the setting of post-liver transplant biopsy, differential diagnosis in this setting includes infection (HSV, CMV), acute cellular rejection, biliary issue (anastomosis stricture), vascular issue (ischemia), etc. While HSV infection leads to hepatocyte necrosis with irregular and randomly distributed pattern, ischemia-associated hepatocyte necrosis occurs at centrizonal areas.
Taken together, a high index of suspicion of adenovirus infection should be maintained especially when evaluating the liver biopsy from pediatric patients with liver transplantation as well as hepatocyte necrosis on microscopic examination.
References:
- Jay H Lefkowitch. Scheuer’s liver biopsy interpretation, 8th, 2010, Saunders. Schaberg KB, Kambham N, Sibley RK, Higgins JPT. Adenovirus Hepatitis: Clinicopathologic Analysis of 12 Consecutive Cases From a Single Institution. Am J Surg Pathol. 2017;41(6):810-819.
Case contributed by: Goo Lee, M.D., Ph.D., Assistant Professor, Anatomic Pathology