Case History
Fine needle aspiration of a left neck mass from a 47-year-old male.
What is the diagnosis?
- Squamous cell carcinoma
- Metastatic carcinoma
- Salivary duct carcinoma
- Mucoepidermoid carcinoma
Answer: B – Metastatic carcinoma (Embryonal carcinoma).
Discussion:
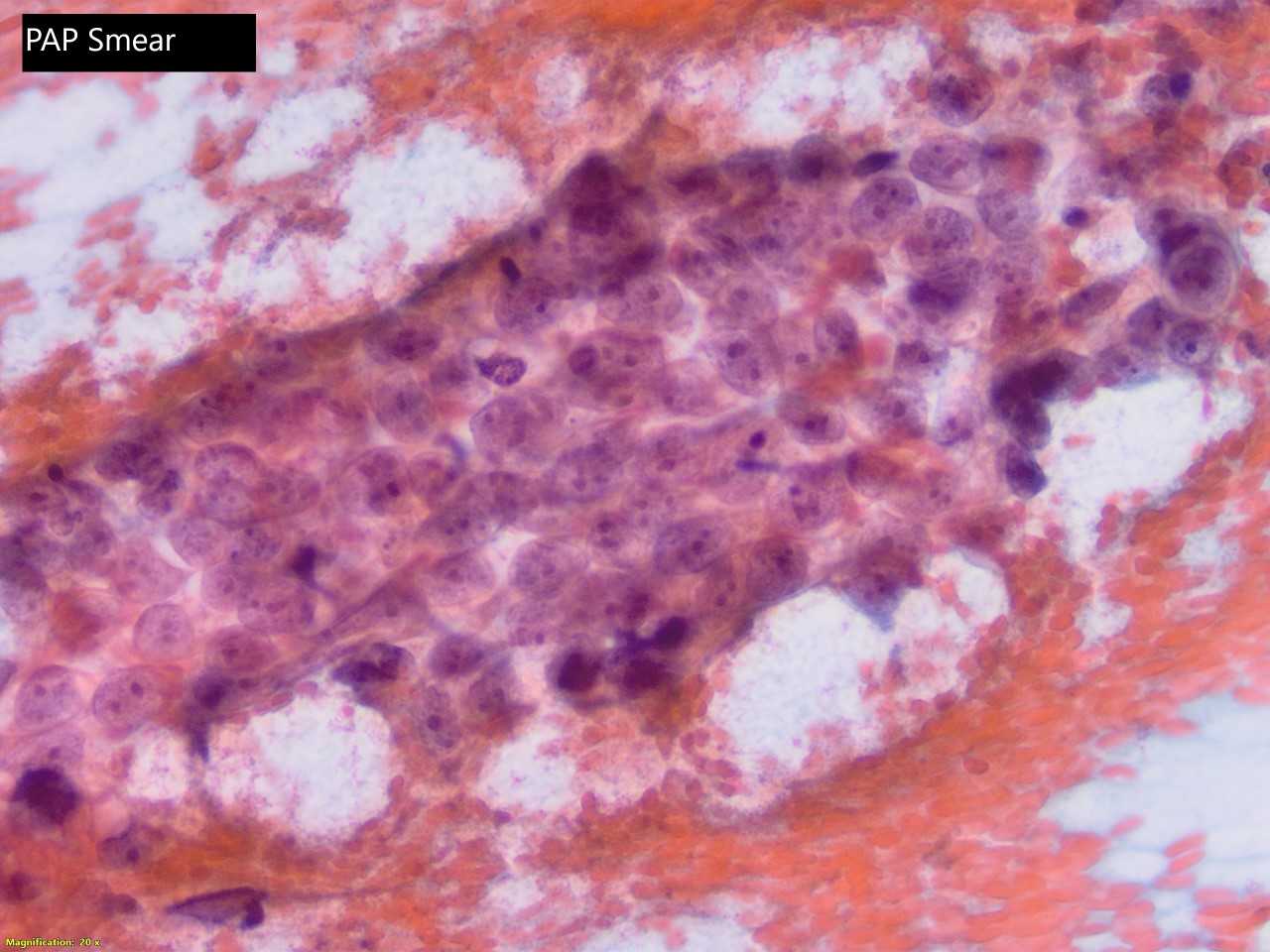
In view of the patient's clinical history of metastatic testicular carcinoma, the morphologic and immunohistochemical profile was most in keeping with a metastatic, germ cell neoplasm. Morphologically and together with the positive OCT3/4, the neoplastic cells were most suggestive of metastatic embryonal carcinoma.
Embryonal carcinoma is an aggressive neoplasm that often presents at an advanced stage of the disease. Histologically is a primitive large neoplasm with marked nuclear anaplasia. Necrosis and hemorrhage are common features.
Cytomorphological features of embryonal carcinoma include tumor cells that have a centrally placed, large, round, or highly irregular nucleus with several nucleoli. The cytoplasm is indistinct and pale. Bizarrely shaped cells and mitoses are common.
A cytological diagnosis of malignancy is straightforward, but distinction from a poorly differentiated carcinoma requires correlation with serological markers and immunocytochemical studies. Embryonal carcinoma, yolk sac tumor, and choriocarcinoma are keratin positive but can be distinguished from epithelial malignancies because of their staining for PLAP and SALL4. Additionally, embryonal carcinoma, like seminoma, is immunoreactive for Oct-3/4 and NANOG. Seminoma can be distinguished from embryonal carcinoma because the former has a characteristic membranous staining pattern for CD117.
Germ cell tumors of the testis usually metastasize to retroperitoneal lymph nodes, lungs, and liver. Other lymphatic or organ metastases especially in the head and neck are rare.
In young men between 20 and 35 years of age with cervical metastases of tumors of unknown primary site, germ cell tumors must be suspected. Histologic findings of non-squamous epithelial metastases (seminoma, embryonal carcinoma, choriocarcinoma, teratoma, yolk sack tumor, and their combined forms) with or without retroperitoneal, mediastinal, or lung metastases; elevated tumor markers (human-chorionic gonadotropin, alpha-feto-protein, placental alkaline phosphatase, lactate dehydrogenase); and palpable intratesticular mass lead to the correct tumor diagnosis. Early detection of the disease is essential for successful therapy and long-term remission.