Case History
A 35 y/o male, with a pathological fracture of the left humerus and a 6.5 cm marrow-replacing lesion.
What is the best diagnosis?
A. Metastatic carcinoma
B. Metastatic melanoma
C. Plastic cell neoplasm
D. Lymphoproliferative disorder
Correct answer: D. Lymphoproliferative disorder
Discussion:
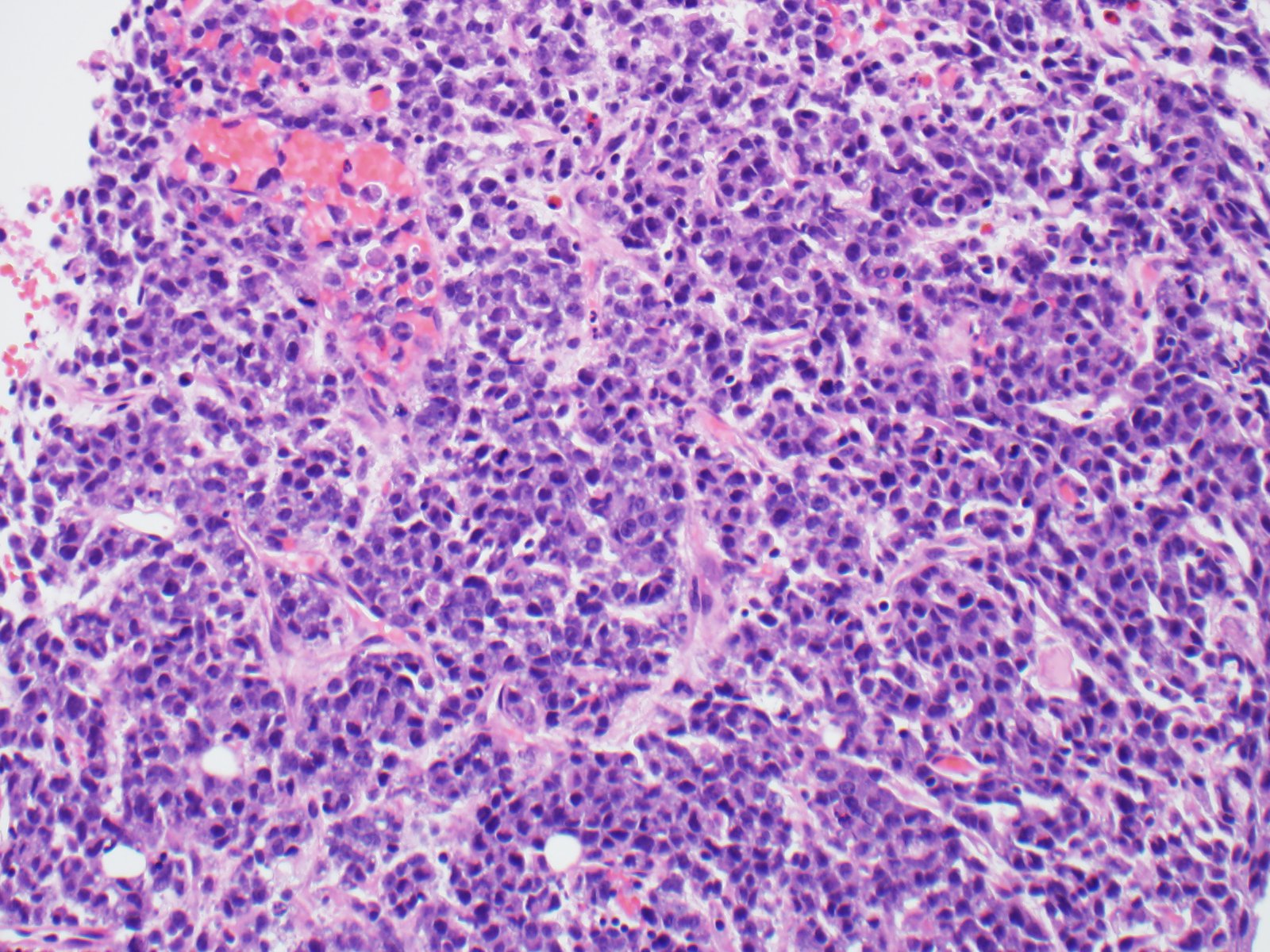
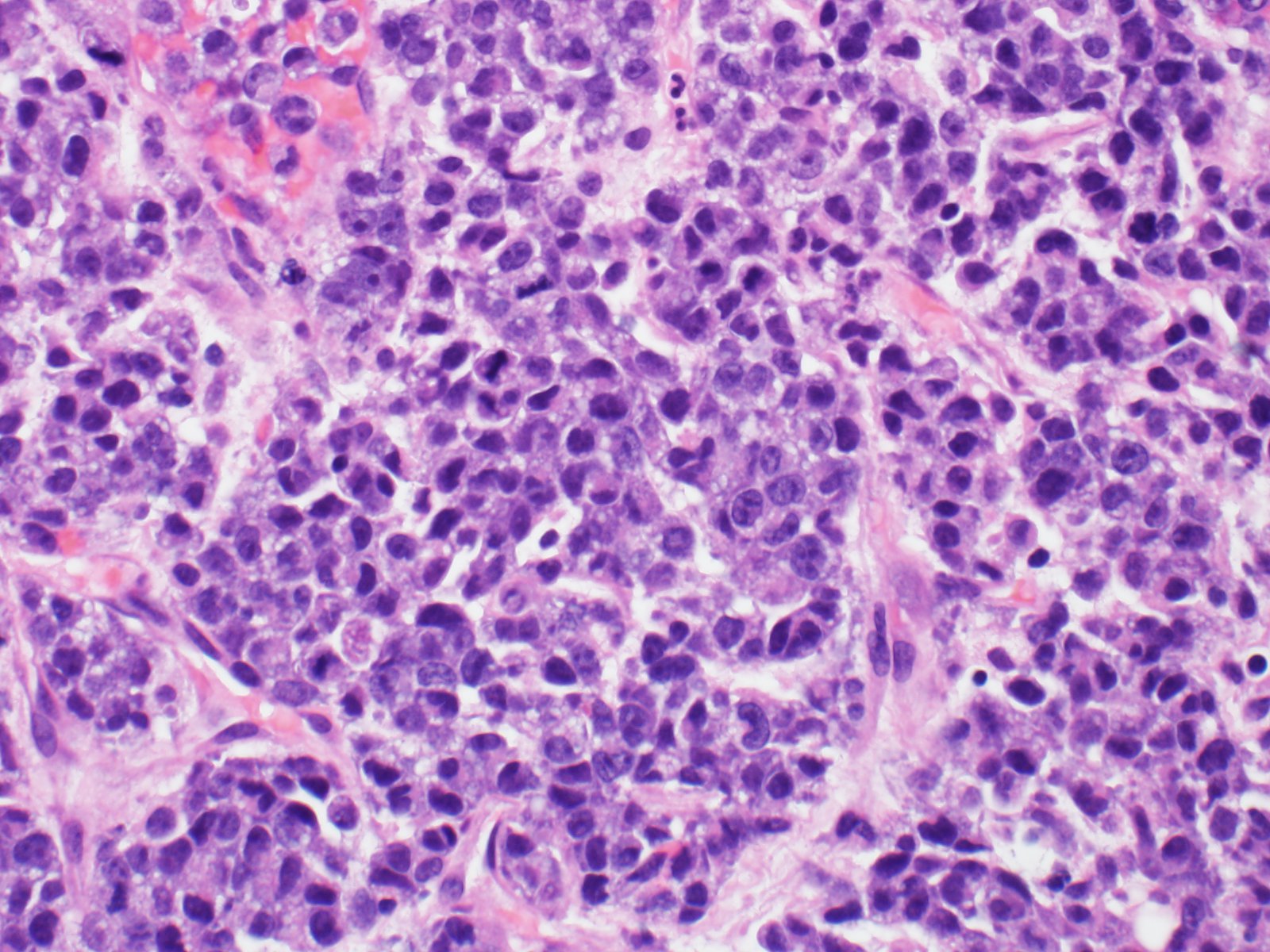
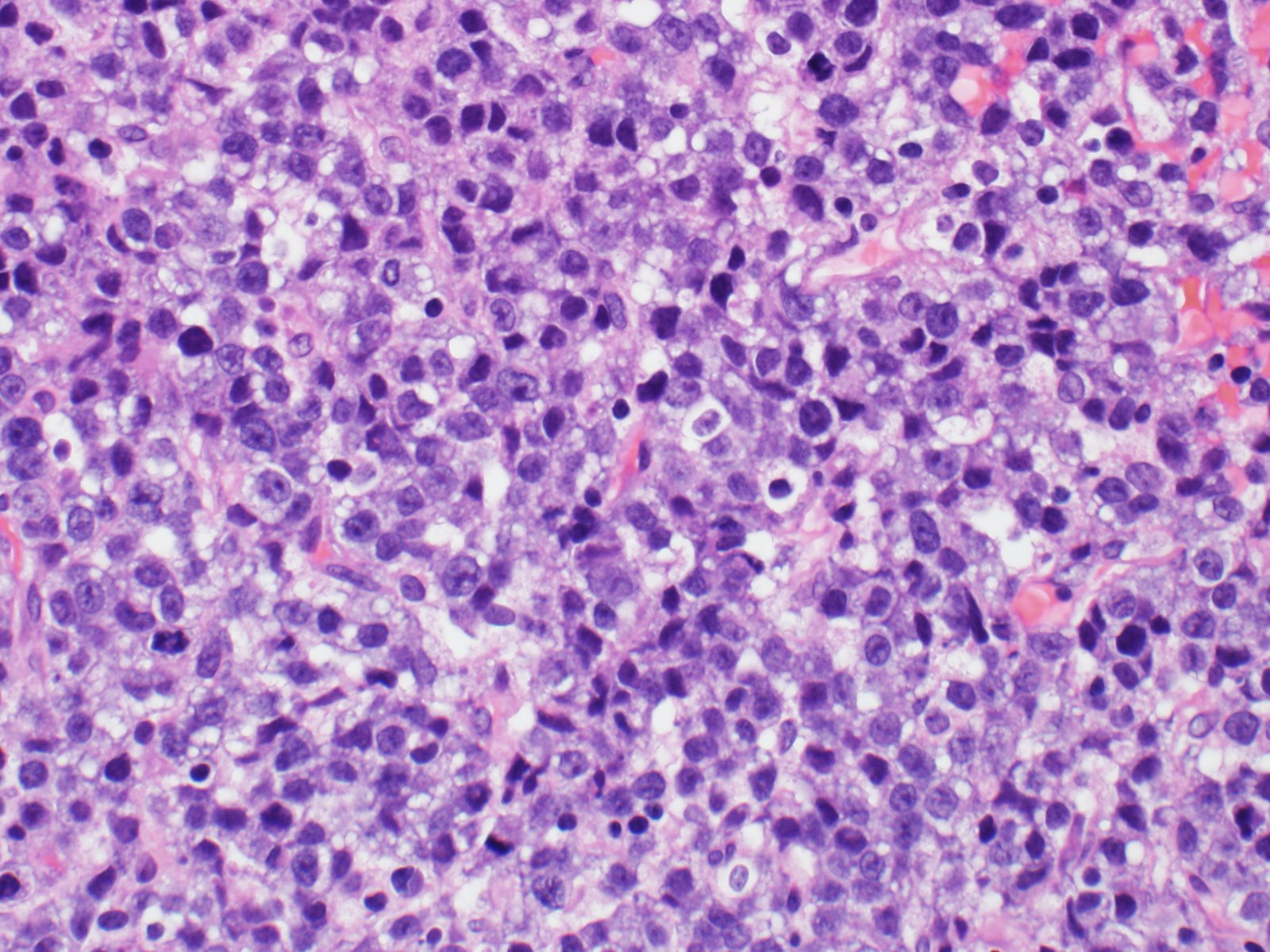
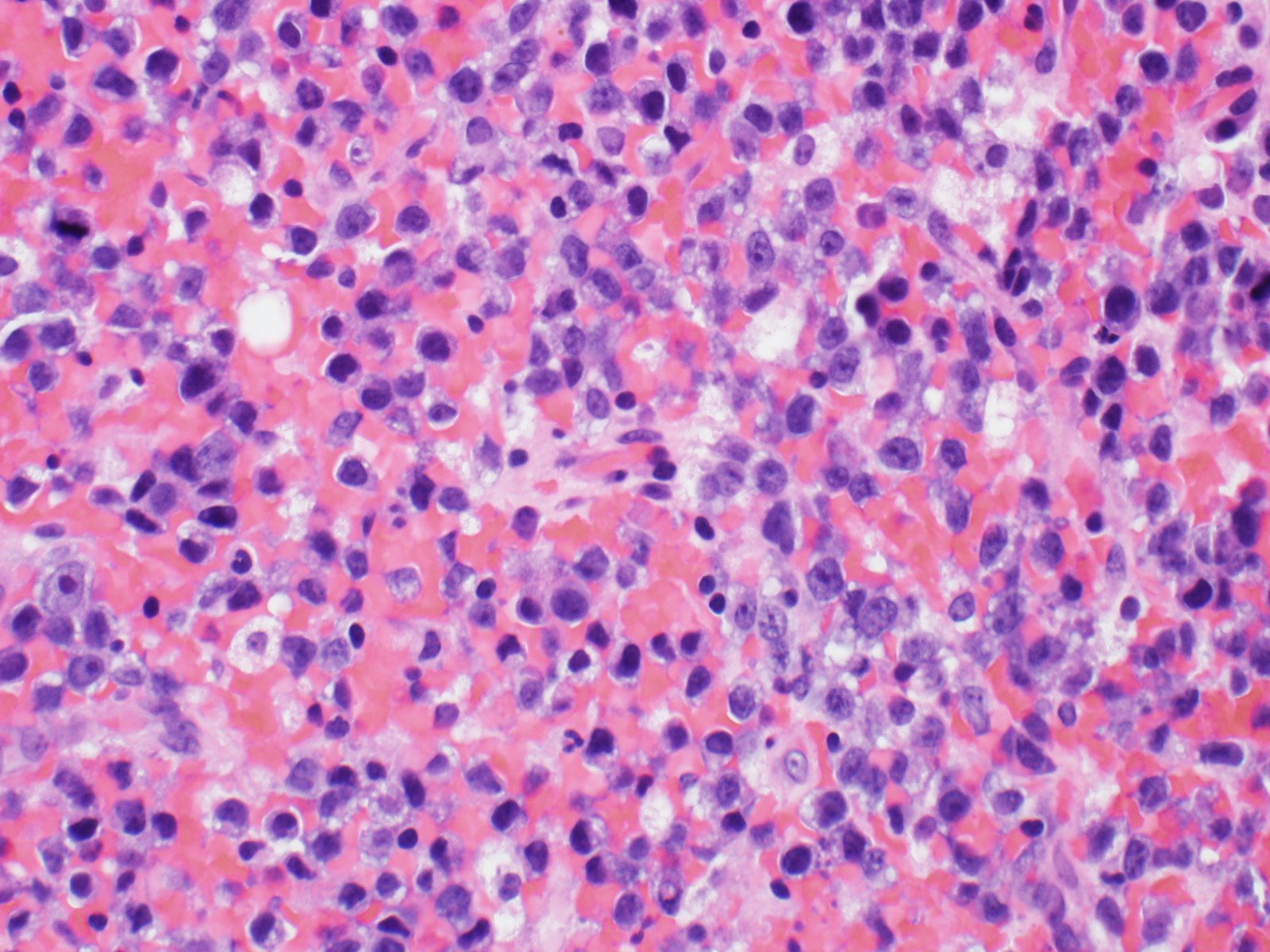
The specimen consists of fragments of bone and a monotonous population of medium-sized atypical cells with prominent nucleoli and scant to moderate amounts cytoplasm that shows some vacuolization. Many cells are round, with occasional kidney-shaped forms. Mitotic figures are readily identified.
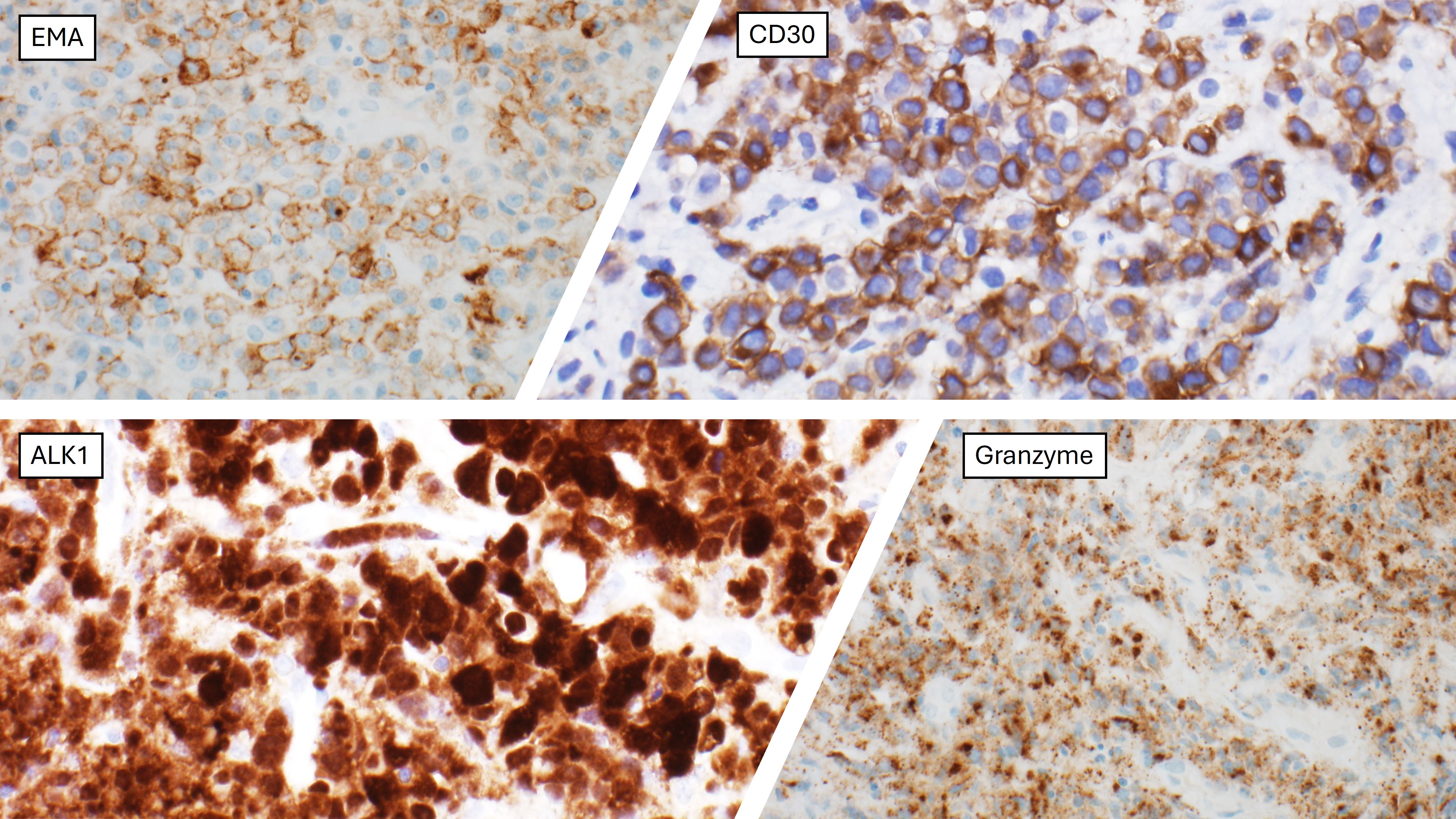
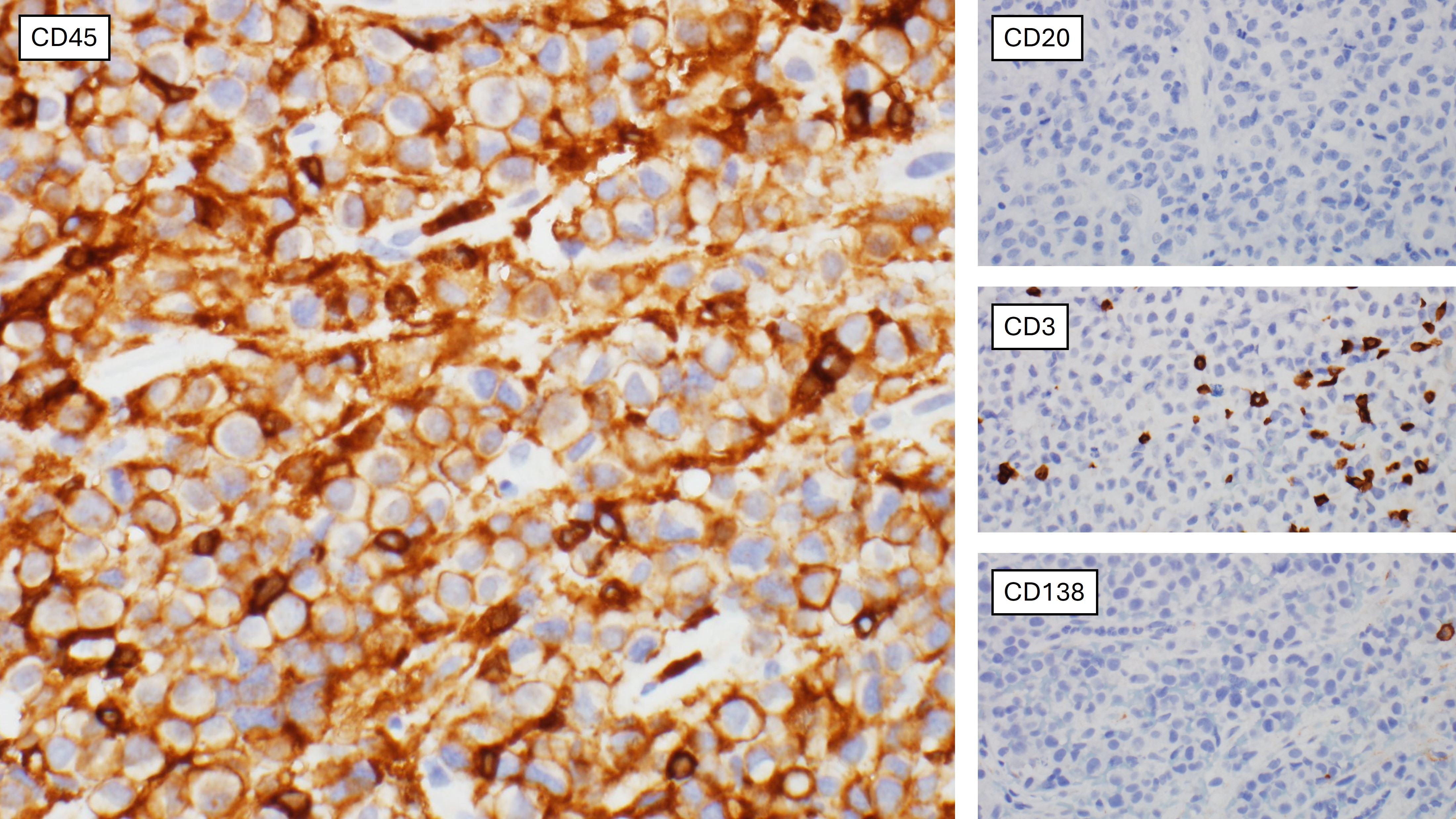
An extensive panel of immunohistochemical stains was performed, as this patient had no prior significant medical history. The cells were diffusely positive for LCA, CD30, EMA and ALK-1, and a subset was positive for CD4 and granzyme. Negative stains included: cytokeratin cocktail, CD99, S100, SOX10, synaptophysin, chromogranin, PAX-8, WT-1, CD2, CD3, CD20, CD79a, PAX5, CD138 and EBER. The final diagnosis was ALK-positive anaplastic large cell lymphoma (ALCL).
ALCL characteristically has a cohesive proliferation of large pleomorphic cells with classic hallmark cells, however there is a broad morphologic spectrum that also includes small to medium sized cells as in this case. Common sites of involvement include lymph nodes and extranodal sites such as skin, bone, soft tissue, lung and liver. The small cell variant of anaplastic large cell lymphoma is a subtype showing unfavorable prognosis which accounts for 6% of ALCLs.
Case contributed by: Frida Rosenblum, M.D., Associate Professor, Anatomic Pathology, UAB Pathology